Are Sex Ratios at Birth Increasing in Vietnam?
Pages 231 to 250
Cite this article
- BÉLANGER, Danièle,
- THI HAI OANH, Khuat,
- JIANYE, Liu,
- LE THANH, Thuy
- and VIET THANH, Pham,
- Bélanger, Danièle.,
- et al.
- Bélanger, D.,
- Thi Hai Oanh, K.,
- Jianye, L.,
- Le Thanh, T.
- and Viet Thanh, P.
https://doi.org/10.3917/popu.302.0255
Cite this article
- Bélanger, D.,
- Thi Hai Oanh, K.,
- Jianye, L.,
- Le Thanh, T.
- and Viet Thanh, P.
- Bélanger, Danièle.,
- et al.
- BÉLANGER, Danièle,
- THI HAI OANH, Khuat,
- JIANYE, Liu,
- LE THANH, Thuy
- and VIET THANH, Pham,
https://doi.org/10.3917/popu.302.0255
Notes
-
[*]
Danièle Bélanger and Liu Jianye: Department of Sociology and Population Studies Center, The University of Western Ontario, London, Canada; Khuat Thi Hai Oanh: Center for Social Development Studies, Hanoi, Vietnam; Le Thanh Thuy, Hanoi Obstetric and Gynecology Hospital, Hanoi, Vietnam; Pham Viet Thanh, Tu Du Obstetric and Gynecology Hospital, Ho Chi Minh City, Vietnam.
-
[1]
A national census was conducted in 1979 but was of poor quality and contained very limited information. For instance, there was no question about marital status.
-
[2]
Geographically, Vietnam is part of Southeast Asia, which is generally characterized by bilateral family systems and more egalitarian gender relations. While there is no agreement as to the relative in?uence of East and Southeast Asian cultures in Vietnam, the historical occupation of Vietnam by China has resulted in the strong in?uence of Confucianism, particularly in the northern and central regions of the country.
-
[3]
According to the 1999 Census data, the total fertility was very similar to the ?gure obtained from the VLSS 1997-98. The census reported 2.0 children per woman, but this number was increased to 2.3 after correction for undercount of children (Le et al., 2001).
-
[4]
While these data refer to live births to women in their reproductive ages, we use the term “families” for clarity. We realize, however, that a woman’s live births may refer to a different reality than the woman’s family at the time of the survey.
-
[5]
Kovac’s method involves the extra-amniotic insertion of a catheter, which is covered by a condom. Saline is then instilled through the catheter to the condom to make it a solution bag. This bag, combined with an intravenous injection of Oxytocin, induces a labour-like abortion in most cases. The mean time from the insertion to the abortion is about 30 hours (Phu San Hospital, 2000). This method is associated with a high risk of infection and other complications (World Health Organization, 1999). It only provides good results for pregnancies 18 weeks and over.
-
[6]
Direct observations by the second author of this paper.
-
[7]
These data were provided by the hospitals to the second author of this paper. They are unpublished.
1The sharp rise in sex ratios at birth in several major Asian countries, such as India and China, is one effect of a persistent strong son preference in a context of rapidly contracting family size. This imbalance to the detriment of girls has been attributed to three factors: under-registration of female births, sex-selective abortion, and excess female mortality in the first year of life related to differences in levels of care. Danièle Bélanger and her colleagues have examined the case of Vietnam, which has cultural affinities with China and has also introduced a family planning programme, the two-child policy, which is strict in its goals though uneven in its application. The data analysed by the authors, including valuable hospital data, do not support the conclusion of a significant increase in sex ratios at birth, although higher ratios are observed in particular social groups (government cadres) and at births of parity 3 and over. If confirmed, this lack of discrimination against girls would attest to a higher status of women in Vietnam than in China.
2Increasing sex ratios in some countries of Asia have attracted considerable attention over the past decade. Beginning with the counts of the world’s “missing daughters” by Amartya Sen (1990) and Ansley Coale (1991), which were estimated to range from 60 to 100 million as of the early 1990s, a signi?cant amount of research has been generated (Aghihotri, 2002; Das Gupta and Bhat, 1997; Klasen and Wink, 2002; Li et al., 2000; Poston et al., 1997). Part of this research explores the causes and consequences of abnormal numbers of males in relation to females. The factors explaining increasing sex ratios at birth have been of particular interest to demographers (Hull, 1990; Li et al., 2000; Park and Cho, 1995; Unisa et al., 2002; Zeng et al., 1993). In the demographic literature, three factors have been identi?ed as explanations for the high sex ratios at birth found in China, South Korea and India: an undercount of infant girls, the use of selective abortion of female foetuses, and the neglect of daughters — infanticide being the extreme form — resulting in higher mortality for girls than boys during the ?rst year of life. The relative importance of each of these factors varies depending on the nature of the country’s population policies, the availability of abortion, access to medical technology for determining the sex of the foetus and differential caring practices for male and female infants. There is a consensus, however, that sex-selective abortion accounts for very high numbers of missing daughters, particularly in Confucian Asia that includes China, Taiwan, Hong Kong and South Korea, where fertility is low and abortion and ultrasound technology are widely available. In contrast, a combination of prenatal and postnatal strategies perpetuates the discrimination against daughters in India (Cohen, 2002; Das Gupta and Bhat, 1997; Sudha and Rajan, 1999; Unisa et al., 2002).
3The underlying cause of high sex ratios at birth is a strong preference for sons. These societies share a patrilineal, patrilocal and patriarchal kinship system, in which sons hold a higher status and have more value to their parents than daughters. Sons are crucial to parents and other kin members for economic, social, cultural and spiritual reasons. While the value of sons as a source of labour has been highlighted for developing societies, the case of South Korea illustrates eloquently that the cultural and spiritual value of sons may persist in the context of socio-economic development (Larsen et al., 1998). In spite of low and declining fertility, son preference remains high and may even be exacerbated because of a clash between a low demand for children — or people’s desire to have a small family — and a high demand for sons (Croll, 2000; Das Gupta and Bhat, 1997). Low fertility can be achieved while the desire for sons may continue to lead the family building process. Without human intervention, however, it is impossible for a large proportion of parents to only have a few children, yet have at least one or two sons. Prevailing, and even increasing, son preference in some Asian societies has been attributed to cultural values that may override the effects of small family size and socio-economic development in promoting greater gender equality among children (Croll, 2000).
4Vietnam shares a similar kinship system and cultural Confucian heritage with China and South Korea. However, little is known about whether sex ratios have increased and whether sex-selective abortions of female foetuses are performed. Vital statistics are incomplete and the ?rst complete census was conducted only in 1989 [1]. In 1999, a new census was conducted and results were made available in late 2001. An examination of the situation in Vietnam, therefore, is now possible and particularly important, since son preference has been clearly identi?ed in demographic research as having a strong in?uence on contraceptive and fertility behaviour in the country (Haughton and Haughton, 1995; Johansson, 1996, 1998). Moreover, abortion is legal and widely available (Goodkind, 1994), and ultrasound technology has been available since the early 1990s. However, no research has focused attention on sex ratios at birth for Vietnam, in spite of its similarity to other countries in which high sex ratios have been documented. This paper begins to address this knowledge gap. The importance of treating this subject also stems from a recent project (December 2002) of the National Committee for Population and Family Planning of Vietnam to draft a law that would forbid sex identi?cation of the foetus through medical technology. In this paper, we present research results on sex ratios at birth from the 1989 and 1999 population censuses of Vietnam, from hospital data for Hanoi and Ho Chi Minh City, and from the 1997-98 Vietnam Living Standards Survey.
I – Demographic behaviour and son preference in Vietnam
5Vietnam features the characteristics of other Asian countries where sex ratios are high: low fertility and a preference for sons. Culturally speaking, Vietnam can be considered part of East Asia, given the strong in?uence of Confucianism [2]. Confucian countries (China, Taiwan, and Korea) have experienced one of the fastest demographic transitions in the developing world (Rele and Alam, 1993). Vietnam is also part of this group because of its rapid fertility decline (Allman et al., 1991; Haughton, 1997) and a high total abortion rate (Goodkind, 1994; Goodkind, 1995a; Henshaw, 1999). With China, Vietnam shares a strong political desire to limit fertility. Since the late 1980s, Vietnam has had a one or two-child policy (Population and Development Review, 1989); however, it is unevenly implemented throughout the provinces and regions of the country (Goodkind, 1995b; San et al., 1999). While ?nes can be substantial in some rural areas, coercion in the form of occupational sanctions and ?nes is mainly enforced on government employees and the military.
6Vietnam’s fertility transition is at a very advanced stage. For the ?rst half of the 1990s (1992-1996), the total fertility estimated by the 1997 Demographic and Health Survey was 2.6 children per woman (National Committee for Population and Family Planning, 1999). Analyses of the 1997-98 Vietnam Living Standards Survey — the most recent source available — show an estimated national total fertility for 1998 of 2.2 children per woman, indicating that Vietnam’s fertility is practically at the replacement level [3] (Le et al., 2001). Fertility has already been below the replacement level for nearly a decade in urban areas and is currently below 3.0 in rural areas (General Statistical Of?ce, 2000b; National Committee for Population and Family Planning, 1999).
7Demographic analyses of fertility and contraceptive behaviour in Vietnam have con?rmed that son preference affects the family building process. Vietnamese families with two daughters are more likely to have a third child than families with at least one son, and women with only daughters are less likely to use contraception than women with one or more sons (Haughton, 1997; Haughton and Haughton, 1995). Furthermore, son preference, as manifested through fertility behaviour, remained strong throughout the 1990s, while the total fertility rate continued to drop (Le et al., 2001). Other research identi?ed a high rate of apparent contraceptive failure experienced by women who had an IUD inserted (Johansson, 1998). In fact, “contraceptive failure” is a common strategy used by couples to hide the secret removal of an IUD in an attempt to have a son while circumventing the two-child policy, a strategy that was also identi?ed in China (Johansson, 1998). Ethnographic research has also documented the strong desire for sons and the much higher status held by sons than daughters, in spite of policies and laws promoting gender equality and a more egalitarian family during four decades of socialism (Bélanger, 2001; Bélanger, 2002b). Vietnam shares many of the characteristics of neighbouring countries where high sex ratios at birth are observed, and prenatal and/or postnatal strategies in favour of sons have been identi?ed.
II – Data and method
8The sex ratio at birth is the ratio of male to female live births. The expected value in human populations is 105 (between 104 and 107), meaning that approximately 105 male infants are born for every 100 female infants. The sex of previous siblings is not thought to in?uence the sex of subsequently born children within families (Jacobsen et al., 1999). Another indicator that is commonly used, as a proxy for the sex ratio at birth, is the sex ratio of the population at age 0, calculated from census data. In this paper, we use three sources of data. First, we use the count of children at age 0, by sex, from the 1989 and the 1999 census results (General Statistical Of?ce, 1992; 2001). For the year 1999, we present ?ndings from the sample results of the census as well. The 1999 sample results are based on a weighted sample of 2 per cent of the households in rural areas and 5 per cent in urban areas (General Statistical Of?ce, 2000a). The sample is statistically representative of the whole population. Because Vietnam divided 15 provinces between 1989 and 1999, the number of provinces increased from 43 to 61 during that decade. For comparative purposes, we merged the newly divided provinces to maintain the same number of provinces for 1999 and for 1989. Two limitations are inherent to the sex ratio of population at age 0 obtained from census data. First, census data are subject to an underreporting of infants, which could be in favour of one sex or the other. Secondly, infant mortality affects the results.
9Vietnam does not provide vital statistics on the sex of children by birth order. In South Korea, it is mainly through analyses of ratios by birth order that the very high ratios have been found (Park and Cho, 1995). These data show an increase for children of higher orders, indicating families’ increasing motivation to have a son as the family building process unfolds. In order to obtain data on sex ratios by birth order, data on all births taking place at two major hospitals, one in Hanoi and the other in Ho Chi Minh City, were collected. Both are among the hospitals performing the highest numbers of deliveries and abortions in these cities. Data were available only for 2001 in Hanoi and for 1996, 1999 and 2001 in Ho Chi Minh City. The total number of births that took place in the hospital in Hanoi was 9,924 in 2001, and, in the hospital in Ho Chi Minh City, it was 31,942 in 1996, 26,893 in 1999 and 29,437 in 2001. Unfortunately, these data sets did not provide information on the sex of previous children born to women.
10In order to capture the effect of both parity and sex of previous children, we used the fertility history component of the 1997-98 Vietnam Living Standards Survey (General Statistical Of?ce, 2000b). This survey is the most recent one providing fertility history data and does so on a random sample of 5,823 married women in their reproductive years (15-49). All women interviewed provided a complete fertility history as well as information on contraceptive use, vaccination of children, prenatal care, and delivery. Based on these data, we estimated sex ratios at birth according to the sex of previously born children. We also compared the theoretical distributions of families by sex composition of children — assuming an independent sex ratio at birth at all parities — to the observed compositions of families. The potential underreporting of births by women interviewed, particularly of children who died early in infancy, is a limitation of survey data for the estimation of sex ratios at birth.
III – Results
1 – 1989 and 1999 censuses
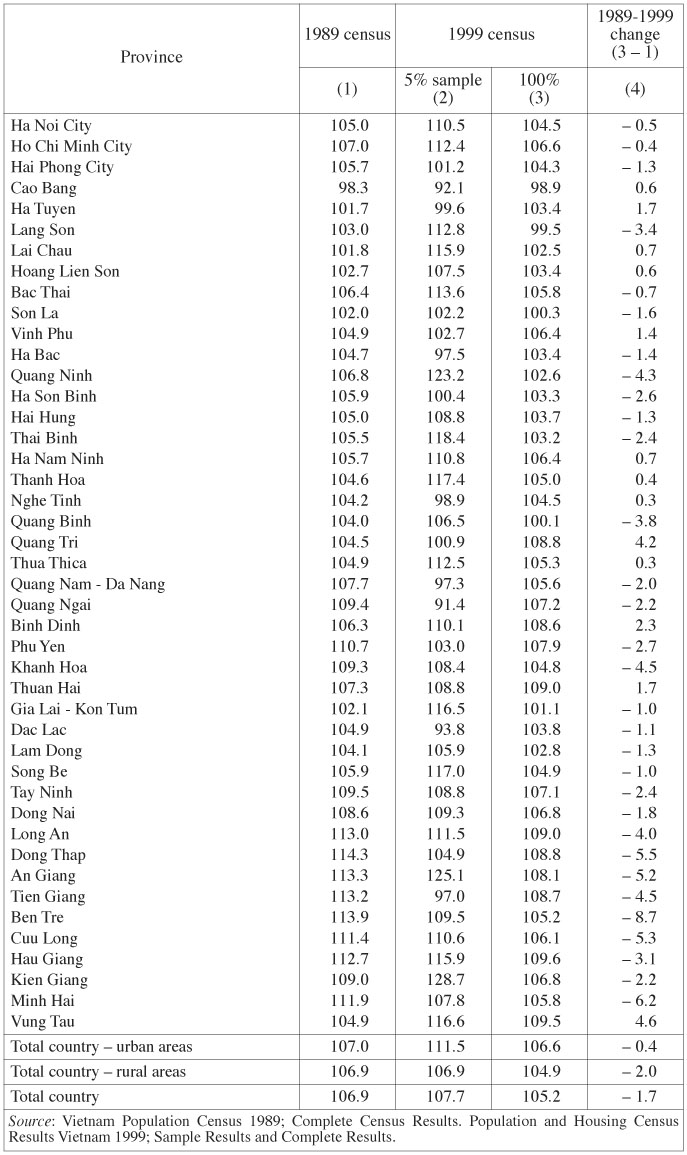
11The sex ratios of the population at age 0 based on the 1989 and 1999 census results are presented in Table 1. Data from the 1989 complete census results are presented in column 1, the 1999 sample results in column 2 and the 1999 complete census results in column 3. In 1989, the national sex ratio at age 0 was 107, still within the expected range of 104 to 107. Data by provinces show that sex ratios were higher in the southern provinces than in the northern ones. Seven provinces located in the south of the country had sex ratios at age 0 above 110. The two provinces where the two largest cities of the country are located — Hanoi and Ho Chi Minh City — had ratios of 105 and 107 respectively. The province of Thai Binh, which has been reported to have forcefully implemented the two-child policy throughout the 1990s (Goodkind, 1995b; Pham et al., 1999; San et al., 1999; Scornet, 2001), had a normal sex ratio at birth of 105 in 1989. Overall, sex ratios are not particularly high, although provinces in the south share a moderately high ratio between 110 and 115.
Sex ratios at age 0 by province and urban or rural residence in Vietnam
Sex ratios at age 0 by province and urban or rural residence in Vietnam
12For 1999, data suggest mixed results, depending on the data set used to calculate the sex ratios among babies less than one year of age. Based on the data from the sample results (column 2), the national sex ratio for 1999 is 107.7, with values varying across provinces. The provinces of Hanoi and Ho Chi Minh have ratios of 110.5 and 112.4 respectively, while the province of Thai Binh has a ratio of 118.4. Overall, 18 provinces have a ratio above 110, the highest being 128.7 in Kien Giang. Following the publication of the sample results in the year 2000, the complete corrected results were published in late 2001. These data were corrected following post-enumeration, which indicated an undercount of children (Le et al., 2001). Such corrections could, however, also have been made for political reasons (see the discussion section below).
13Ratios calculated on the complete census results for 1999 (column 3) indicate lower sex ratios at age 0 than in the sample results, with the national ?gure being 105.2. No province has a ratio above 110. For 27 provinces, the ratio decreased following correction, and it increased in the 17 remaining ones. In all cases except one, the increase is for provinces that had a sex ratio below 105 in the sample results. In addition, ratios from the complete results of the 1999 census are lower than in 1989 in 31 of the 44 provinces. According to these data, sex ratios for 1999 are normal in the vast majority of provinces. In 9 provinces they are between 108 and 110. These provinces are located in the center and south of the country.
14Based on the complete results of the 1989 and the 1999 censuses, the question remains open as to whether or not sex ratios among infants are increasing in Vietnam. If we compare the complete results for the two census years, they indicate a decrease, which is a rather unlikely trend given the relationship found elsewhere between declining fertility and son preference. In the set of questions on fertility answered by women in their reproductive ages, the 1999 census collected data on the total number of births and on the sex of the lastborn child only (as opposed to the sex of all already born children). As shown in Table 2, sex ratios for lastborn children increase with the age of the mother from 107 for women aged 2024 to 110 for women aged 35-39. This result appears logical, since older women are more likely to have higher-parity children and have a higher motivation to have a son. The increase, however, remains modest and is not apparent in women aged 40-44. The high ratio of 139 for women aged 45-49 years is probably calculated on a small number of births (numbers are not provided in census documents; see General Statistical Of?ce, 2000, p. 186).
Sex ratios of lastborn child by age of mother

Sex ratios of lastborn child by age of mother
2 – Hospital data on births for Hanoi and Ho Chi Minh City
15Data for the hospital in Hanoi for the year 2001 are shown in Table 3. The sex ratio based on the total number of births is 103.9. Sex ratios at birth increase sharply with birth order. At orders 3 and 4, ratios are 147 and 223 respectively (data not shown). When combining births of parity 3 and over, the sex ratio at birth is 156.4. These data indicate that more sons than expected are born at higher parities.
Sex ratios of live births by parity in hospital data from Hanoi and Ho Chi Minh City

Sex ratios of live births by parity in hospital data from Hanoi and Ho Chi Minh City
16The sex ratios for all births recorded in the hospital in Ho Chi Minh City are generally above 107 and declined from 109.5 to 107.5 between 1996 and 2001, as shown in Table 3. Sex ratios by birth order do not increase from parity one to three; however, ratios are generally above 107 for the ?rst and second child. The highest is observed for the third birth order at 110.7 in 1996. Overall, these data do not suggest that sex ratios are increasing across the three years of observation and by birth order. Higher ratios for the ?rst and second born could indicate that couples who are motivated to have few children, but at least one son, may use strategies to sex-select their children at the early stage of the family building process. A similar ?nding has been documented by Park and Cho (1995) among small urban families in South Korea.
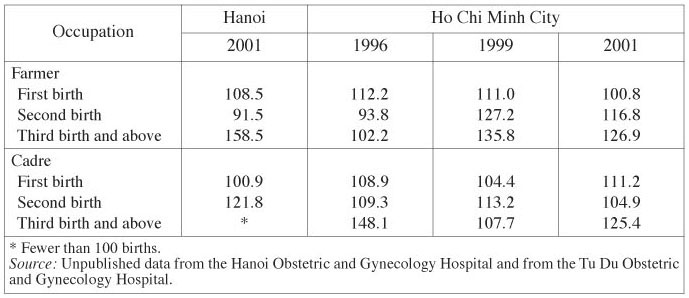
17The hospital data also provide information on the mother’s occupation. Such information is relevant because some individuals are under less pressure to abide by the two-child policy than others. Previous research has indicated that cadres and government workers are more likely to incur sanctions for not respecting the two-child policy and are, therefore, likely to experience much more pressure than others to achieve a family of two, while producing at least one son (Bélanger, 2001; Bélanger, 2002b; Goodkind, 1995b). As a result, they may be more inclined to sex-select their children. Table 4 presents the sex ratios at birth by mother’s occupation in the hospitals studied. In Hanoi, cadres and workers have the highest sex ratios — but still within the normal range — when all births are considered. By birth order, the effect of mother’s occupation is apparent for the second birth order for cadres (121.8). (Data are not shown for all occupations; see Table 5 for data on cadres and farmers). For children of parity 3 and over born in Hanoi (year 2001), ratios by occupation are the highest for farmers (158). Since the analysis for parity 3 and over by occupation involves a small number of births in Hanoi, the ?ndings should be interpreted with caution.
18In Ho Chi Minh City, data by mother’s occupation do not suggest any trend across the three years of observation, as shown in Table 4. In 2001, the ratios for farmers and cadres were higher than 107 (111.0 and 109.9). These data do not show any clear pattern with respect to differential behaviour of mothers with different occupations at the time of birth. Data by occupation and birth order for Ho Chi Minh City, however, do suggest that at the third parity, farmers and cadres have children with a high sex ratio at birth, as shown in Table 5. Such an effect was not apparent in Table 3 when all births were considered. Table 5 suggests that occupation does matter in Ho Chi Minh City, and, given the greater numbers of births recorded there, analyses by occupation and birth order are more reliable than those for Hanoi.
Sex ratios of live births by occupation of the mother in hospital data from Hanoi and Ho Chi Minh City

Sex ratios of live births by occupation of the mother in hospital data from Hanoi and Ho Chi Minh City
Sex ratios at birth by occupation of the mother (cadre and farmer only) and parity
Sex ratios at birth by occupation of the mother (cadre and farmer only) and parity
19Overall, data on hospital births indicate that in Hanoi, sex ratios at birth increase with birth order, while there is no evidence of such a trend in Ho Chi Minh City. For both cities, mothers who are cadres tend to have higher sex ratios at birth for children of third and higher birth orders. We also see a higher sex ratio by birth order for farmers in Hanoi in 2001 and in Ho Chi Minh City in the two most recent years for which we have data (1999 and 2001).
3 – The 1997-98 Vietnam Living Standards Survey
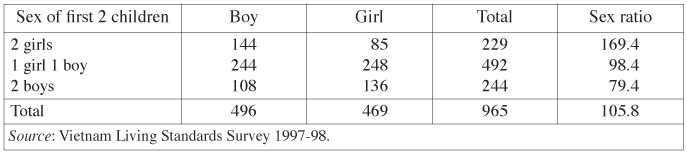
20Data from the Vietnam Living Standards Survey provide strong support for the hypothesis that Vietnamese families having more than two children are willing to use strategies to in?uence the sex of the children to be born. Using information on all live births among 965 women who had three children at the time of the survey, the sex ratio of the third child was estimated. Results shown in Table 6 indicate that women who had two daughters ?rst have a much higher likelihood of having a son as their third child (sex ratio of 169.4) than women who had a boy and a girl (sex ratio of 98.4) or two sons (sex ratio of 79.4). Interestingly, the low sex ratio for the third birth among women who had two sons suggests a desire for one daughter. The desire for both a son and a daughter has been identi?ed in fertility analyses done by Haughton and Haughton (1999) on the basis of the 1992-93 Vietnam Living Standards Survey data.
Sex ratios at third birth by previous sex distribution of children born to women
Sex ratios at third birth by previous sex distribution of children born to women
21In Table 7, the theoretical distributions of different family compositions by sex (assuming that the sex ratio at birth is independent of children previously born) are compared with the observed distributions [4]. Differences observed between the two distributions are statistically signi?cant. We restrict the analysis to women who had one, two or three live births, given the low proportion of women who had more than three live births. Overall, families with sons are more frequent, and families with daughters less frequent than expected. Among three-child families, women with two daughters and one son are more common than expected theoretically (+ 4.1 points), and families with three daughters less common (– 2.8 points). Interestingly, families with three sons are 2.2 points less common than expected. A family composed of two daughters has the largest difference between the expected and the observed distributions (– 5.3 points). This result could indicate that couples under pressure to respect the two-child limit are more likely to attempt in?uencing the sex of their second child. While the differences between the expected and the observed distributions are statistically signi?cant as a whole, differences remain small. These data do not consider the birth order of children by sex, only the sequence of births by sex.
Theoretical and observed sex distribution of children born to women

Theoretical and observed sex distribution of children born to women
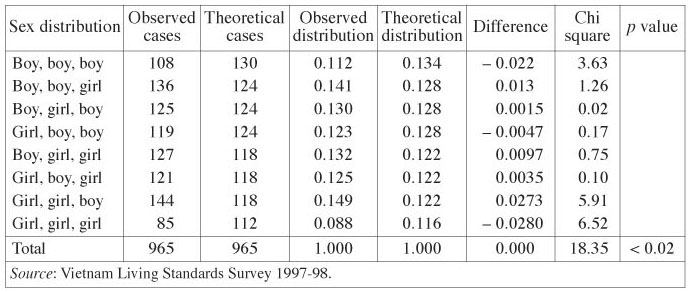
22In Table 8, information on the sex of children of women who had only three live births is used to compare the theoretical with the observed frequencies of family composition (including birth order by sex). These results are statistically signi?cant (p < 0.02) and indicate that the sex of the third child is affected by the sex of the two ?rst children. As observed in the previous table, families consisting of three children of the same sex, male or female, are less common than expected. However, those who have two daughters ?rst are more likely than expected to have a son as their third child than women who had two sons ?rst are to have a daughter as their third child.
Theoretical and observed sex distribution of children born to women, by birth sequence
Theoretical and observed sex distribution of children born to women, by birth sequence
IV – Discussion
23Overall, our results do not provide clear evidence that the national sex ratio at birth is increasing in Vietnam. From the census data, one could conclude that the clash between son preference and a desire for a small family size has not led to increasing sex ratios at birth (sex ratios of the population at age 0), as it has in China (Lavely, 2001). The fact that sex ratios of the population at age 0 by province have declined between 1989 and 1999 is nonetheless puzzling, given the regional trend. In fact, the discrepancy between the sample and the complete results (by province) of the 1999 population census raises important questions with respect to data quality and the nature of the adjustments made to the complete results. Political factors may have in?uenced these adjustments. The publication of unbalanced sex ratios can have important political consequences internally and abroad. In January 2003, a Population Ordinance was passed prohibiting sex selection of the foetus by any means. The legal document includes provisions for punishments, ?nes and criminal charges for those violating the law (article 38). It may be that the sample results, in spite of their irregularities, are closer to reality than the complete results; in fact, it has been suggested that the sample results had prompted the legal initiative. However, such hypothesis is speculative and the question as to whether or not sex ratios at birth are increasing in Vietnam remains open. To be sure, the existence of sex-selective abortions has received very little attention in Vietnam and remains more or less a taboo issue. The vast majority of medical practitioners, researchers and policy makers to whom we talked about this research were prompt in stating that sex-selective abortions did not exist in Vietnam, while they unanimously recognized the strong demand for ways to conceive and deliver sons.
24In contrast to national data, hospital and survey data do indicate abnormal sex ratios at birth among some groups of the Vietnamese population. Data on hospital births suggest that in the north sex ratios at birth increase with parity, while no such trend is apparent in the south. The effect of occupation on sex ratios at birth indicates that cadres and farmers tend to have higher sex ratios at birth, particularly at higher parities. These results coincide with studies on the implementation of the family planning programme that show that cadres in particular are under pressure to respect the two-child limit.
25The survey data analyzed show that the sex ratio at birth increases with parity among women with daughters only. Results from the Vietnam Living Standards Survey of 1997-98 point to an interesting fact: families with three children of the same sex are less common than expected. One could surmise that having three sons would be desirable; however, according to our ethnographic material (Bélanger, 2002b), rural peasants of the north avoid having three sons. Parents fear that having to divide residential land among three sons would result in the creation of three extremely small plots of land. Hence, the stopping rule prevailed in this village, and the fear of having too many sons prevented couples with two sons from attempting to have a daughter. Those having two sons are also more likely to stop childbearing to avoid any problems for not respecting the population policy.
26Three main factors have been identi?ed in the literature on the varying sex ratios at birth in Asia. The ?rst one, an underreporting of female babies, has been identi?ed as being important in the Chinese case given the stringent population policy leading families to hide the birth of daughters, or to give them up for adoption and not to report them as live births. A systematic undercount of female children in Vietnam appears unlikely in the censuses and in the 1997-98 Vietnam Living Standards Survey. Unlike in China, the notion of children born without permission does not exist, and Vietnam’s one or two-child policy does not encompass sanctions that will directly affect the lives of children born at order 3 or higher, such as limited access to health care and education. While workers may suffer more than peasants for violating the policy, all are generally ?ned a certain amount of paddy or money. The amount, however, varies and, in some rural areas, it may not be collected until several years after the birth of the child. The nature of the family planning policy and the relative leniency with which the two-child limit is implemented in some provinces should not lead to a systematic underreporting of baby girls. Nevertheless, it is possible that some families have omitted to report daughters in order to give the impression that they were respecting the policy. To be sure, more analyses are needed to evaluate the accuracy in the reporting of children by sex. Studies are also necessary to investigate other types of behaviour, such as the adoption of female children, which may affect the reporting of daughters.
27The second possible factor accounting for high sex ratios at birth is the higher mortality of girls resulting from differential care and treatment in early infancy. In India for instance, discrimination against daughters that results from son preference is manifested by the higher probability of death for girls, in spite of the fact that male infants are biologically more likely to die than female infants (Das Gupta, 1999; Das Gupta and Bhat, 1997). In the case of Vietnam, however, most research on demographic and health outcomes suggests that, once born, sons and daughters are not treated differently (Bélanger, 2002a). Nutritional status does not vary by sex, and parental use of health care services is not inferior for daughters (Haughton and Haughton, 1997). Mothers breastfeed sons and daughters for an equal amount of time (National Committee for Population and Family Planning, 1999; Swenson, 1993), and gender is not a signi?cant variable for explaining differences in vaccination coverage (General Statistical Of?ce, 2000b). In general, ethnic group and socioeconomic status, rather than gender, account for observed differences in infant mortality. Much research provides evidence that the probability of death in early infancy for each sex is normal (Swenson, 1993; The World Bank, 2001). We estimated infant mortality rates from the Vietnam Living Standards Survey of 1997-98 (using the fertility history data) and found that, among all infant deaths recorded, the infant mortality rate was 47.9 per 1,000 for boys and 39.3 per 1,000 for girls.
28Finally, the last potential factor accounting for high sex ratios at birth is the practice of using ultrasound or other techniques to determine the sex of the foetus, then subsequently procuring a sex-selective abortion. Abortion has been legal in Vietnam since 1954, and during the late 1980s, abortion services were expanded and services from private providers were legalized. Data published by the Ministry of Health suggest very high abortion rates, with a rapid increase in the early 1990s (Goodkind, 1994). A more recent source, also relying on government statistics, estimated Vietnam’s total abortion rate to be 2.5 per thousand people for 1996, the highest among all developing countries of the world (Henshaw, 1999). In 1996, there were 43.7 abortions per 100 known pregnancies (Henshaw, 1999). In spite of these high numbers, most abortions are performed during the ?rst term of pregnancy, since second-term abortions are dif?cult to obtain in Vietnam. Government statistics on abortion do not even include data on second-term abortions. Furthermore, data indicate that second-term abortions performed in major hospitals are on the decline due to the providers’ hesitations to use a technique that is neither safe nor guaranteed. This technique is called Kovac’s method [5]; it is the only method currently approved by the Ministry of Health for second-trimester abortion in Vietnam. One of the two leading obstetrical hospitals in Hanoi used to perform second-term abortions, but no longer does so. Similarly, many tertiary hospitals no longer provide this service. In a large obstetrical hospital located in the south, many women who come for second-trimester abortions are convinced to carry on with their pregnancy and give the child up for adoption. This hospital even provides accommodation for those who wish to stay in the hospital until delivery [6]. In that hospital, the annual number of second-term abortions declined from 970 to 548 between 1998 and 2001, corresponding to 2.8% to 1.8% of all abortions performed. Data on a hospital of the Quang Ninh Province show higher proportions of abortions performed during the second term, but also a steeper decline from 12.6% to 7.5% of all abortions [7].
29Ultrasound technology was introduced in the early 1990s and has become widespread in major hospitals since the mid-1990s. All provincial and central level hospitals currently have ultrasound machines, and some hospitals own 3-D machines in the largest urban areas. In recent years, major investments in the health sector have provided district health centers with ultrasound machines. No data on the number of ultrasound machines is available; however, by the end of the year 2001, the Imaging Diagnostic Department of the Hanoi Medical School estimated that the vast majority of district health centers of the country were equipped with at least one ultrasound machine. Ultrasound technology is also provided privately in the major cities of the country.
30However, since the identi?cation of the sex of the foetus by ultrasound is more accurate during the second term of the pregnancy, and since second-term abortions are dif?cult to obtain, the number of women who can resort to this strategy remains limited. This could explain the fact that Vietnam’s national sex ratios at birth remain normal, in spite of a combination of elements, including low fertility, son preference and the availability of ultrasound technology and abortions which have led to a more widespread use of sex-selective abortions elsewhere.
31Another explanation for the national sex ratio at birth apparently not increasing between the two census years could be a different reaction to the strong desire to have a son for the Vietnamese population than among the Chinese. Perhaps the majority of Vietnamese people are less inclined to take action when their reproductive desires are not ful?lled by nature. The intensity of son preference, of course, is dif?cult to compare from nation to nation, but the fact that the national sex ratio does not seem to increase could be a sign that son preference in Vietnam is not as strong as in China or India. Research on gender, pointing to a higher status of women in Vietnam than in China, could, in fact, suggest that Vietnamese women and couples are reluctant to eliminate already conceived daughters. In other words, if the census results are accurate, Vietnam is either lagging behind or responding differently to son preference in the context of low fertility. In light of our results from the hospital and the survey data, however, one could question the accuracy of the census data.
Conclusion
32Vietnamese census data of 1989 and 1999 do not indicate that the sex ratios at age 0 are abnormal or increasing in Vietnam. However, a more detailed analysis of survey and hospital data does indicate that sex ratios at birth by parity and by the sex of children previously born are higher than expected. Taking the mother’s occupation into account reveals that some segments of society — namely government cadres — appear more motivated or pressured to in?uence the sex of children to be born. Vietnam’s preference for sons has been con?rmed by fertility and contraceptive behaviour, as well as by ethnographic studies on the value of children. However, son preference and the discrimination against daughters do not appear to be as important in Vietnam as they are in China, India and South Korea.
33While current sex ratios at birth, based on hospital data, suggest that some Vietnamese families may resort to sex-selective abortion in Hanoi, we have no evidence to con?rm this hypothesis. It seems that Vietnam, with its generally non-coercive two-child policy, has managed to limit discrimination against daughters. However, the desire for a small family size, combined with the increasing availability of ultrasound technology and other ways to in?uence the sex of children, may exacerbate the desire for sons in the near future. The reduction in services for second-term abortions could counteract the desire to use sex-selective abortion as a strategy to achieve a desired family composition. But this phenomenon could lead to a ?ourishing private sector offering second-term abortions if there was a demand. We shall not discard a potentially different response from the Vietnamese population to the clash between a declining fertility and a desire for sons. Much research remains to be done on son preference in a low-fertility regime and the potential implications for the sex structure of the population, gender inequalities among children, and family and kinship systems.
Acknowledgements
The Social Science and Humanities Research Council of Canada provided the funding for this research. The authors thank Dr T.R. Balakrishnan for his comments on a previous version of this paper.REFERENCES
- Aghihotri S., 2002, “Setting daughters of urban India: locating the epicentres of female de?cit”, Paper presented at the Symposium on Sex Ratio in India, January 2002, New Delhi.
- Allman J., Nha V. Q., Minh N., San P. B., Man V. D., 1991, “Fertility and family planning in Vietnam”, Studies in Family Planning, 22, pp. 308-317.
- Bélanger D., 2001, “Son preference and demographic change in Vietnam”, Paper presented at the XXIVth IUSSP General Population Conference, Salvador de Bahia, Brazil, August 2001.
- Bélanger D., 2002a, “Childhood, gender and power in Vietnam”, in H. Lansdowne, P. Dearden, W. Neilson (eds), Communities in Southeast Asia: Challenges and Responses, Victoria, Center for Asia-Paci?c Initiatives.
- Bélanger D., 2002b, “Son preference in a rural village in North Vietnam”, Studies in Family Planning, 33, pp. 321-334.
- Coale A., 1991, “Excess female mortality in the balance of sexes in the population: an estimated number of missing females”, Population and Development Review, 17, pp. 517-523.
- Cohen A., 2002, “Excess female mortality in India: the case of Himachal Pradesh”, American Journal of Public Health, 90, pp. 1369-71.
- Croll E., 2000, Endangered Daughters. Discrimination and Development in Asia, London, Routledge.
- Das Gupta M., 1999, “Gender Bias in China, South Korea and India 1920-1990”, Development and Change, 30, pp. 619-652.
- Das Gupta M., Bhat M. P. N., 1997, “Fertility decline and increased manifestation of sex bias in India”, Population Studies, 51, pp. 307-315.
- General Statistical Office, 1992, Vietnam Population Census 1989. Completed Census Results, Hanoi, Statistical Publishing House.
- General Statistical Office, 2000a, Population and Housing Census Vietnam 1999. Sample Results, Hanoi, Nha Xuat Ban The Gioi.
- General Statistical Office, 2000b, Vietnam Living Standards Survey 1997-1998, Hanoi, Statistical Publishing House.
- General Statistical Office, 2001, Population and Housing Census Vietnam 1999. Completed Census Results, Hanoi, Statistical Publishing House.
- Goodkind D., 1994, “Abortion in Vietnam: measurements, puzzles, and concerns” (in report), Studies in Family Planning, 6, pp. 342-352.
- Goodkind D., 1995a, “Rising gender inequality in Vietnam since reuni?cation”, Paci?c Affairs, 68, pp. 342-359.
- Goodkind D., 1995b, “Vietnam’s one-or-two-child policy in action”, Population and Development Review, 21, pp. 85-111.
- Haughton D., Haughton J., 1997, “Explaining child nutrition in Vietnam”, Economic Development and Change, 45, pp. 541-556.
- Haughton J., 1997, “Falling fertility in Vietnam”, Population Studies, 51, pp. 203-211.
- Haughton J., Haughton D., 1995, “Son preference in Vietnam”, Studies in Family Planning, 26, pp. 325-338.
- Haughton J., Haughton D., 1999, “Son preference”, in J. Haughton et al. (eds), Health and Wealth in Vietnam, Singapore, Institute of Southeast Asian Studies.
- Henshaw S., 1999, “Incidence of abortion worldwide”, International Family Planning Perspectives, 25 (supplement), pp. S30-S38.
- Hull T. H., 1990, “Recent trends in sex ratios at birth in China”, Population and Development Review, 16, pp. 63-83.
- Jacobsen R., Moller H., Mouritsen A., 1999, “Natural variation in the human sex ratio”, Human Reproduction, 14, pp. 3120-3125.
- Johansson A., 1996, “Family planning in Vietnam - women’s experiences and dilemma: a community study from the Red River Delta”, J. Psychosom. Obstet. Gynecol., 17, pp. 59-67.
- Johansson A., 1998, “Population policy, son preference and the use of IUDs in North Vietnam”, Reproductive Health Matters, 6, pp. 66-76.
- Klasen S., Wink C., 2002, “A turning point in gender bias in mortality? An update on the number of missing women”, Population and Development Review, 28, pp. 285-312.
- Larsen U., Chung W., Das Gupta M., 1998, “Fertility and son preference in Korea”, Population Studies, 52, pp. 317-325.
- Lavely W., 2001, “First impressions from the 2000 census of China”, Population and Development Review, 27, pp. 755-770.
- Le V. D., Haughton D., Haughton J., Do A. K., Le D. K., 2001, “Fertility decline”, in D. Haughton, J. Haughton (eds), Living Standards and Economic Boom. The Case of Vietnam, Hanoi, Statistical Publishing House.
- Li N., Feldman M. W., Shuzhuo L., 2000, “Cultural transmission in a demographic study of sex ratio at birth in China’s future”, Population Biology, 56, pp. 161-172.
- National Committee for Population and Family Planning, 1999, Demographic and Health Survey 1997, Hanoi, National Committe for Population and Family Planning.
- Park C. B., Cho N.-H., 1995, “Consequences of son preference in a low-fertility society: imbalance of the sex ratio at birth in Korea”, Population and Development Review, 21, pp. 59-84.
- Pham B. S., Ross J. A., Nguyen L. P., Nguyen D. V., 1999, “Measuring family planning program effort at the provincial level: a Vietnam application”, International Family Planning Perspectives, 25, pp. 4-9.
- Phu San Hospital, 2000, Review of 105 Kovac’s Cases in Phu San Hospital, Hanoi.
- Population and Development Review, 1989, “Vietnam’s new fertility policy”, Population and Development Review, 15, pp. 169-172.
- Poston Jr. D. L., Gu B., Liu P. P., McDaniel T., 1997, “Son preference and the sex ratio at birth in China: a provincial level analysis”, Social Biology, 44, pp. 55-76.
- Rele J. R., Alam I., 1993, “Fertility transition in Asia: the statistical evidence”, in R. Leete, I. Alam (eds), The Revolution in Asian Fertility. Dimensions, Causes, and Implications, Oxford, Clarendon Press.
- San P. B., Ross J. A., Nguyen L. P., Nguyen D. V., 1999, “Measuring family planning program effort at the provincial level: a Vietnam application”, International Family Planning Perspectives, 25, pp. 4-9.
- Scornet C., 2001, “An example of coercive fertility reduction, as seen in the region of the Red River Delta in Viet Nam”, Population: An English Selection, 13(2), pp. 101-134.
- Sen A., 1990, “More than 100 million women are missing”, New York Review of Books, pp. 61-65.
- Sudha S., Rajan S. I., 1999, “Female demographic disadvantage in India 1981-1991: sex selective abortions and female infanticide”, Development and Change, 30, pp. 585-618.
- Swenson I. E., 1993, “Factors in?uencing infant mortality in Vietnam”, Journal of Biosocial Science, 25, pp. 285-302.
- The World Bank, 2001, Vietnam Growing Health: A Review of Vietnam’s Health Sector, The World Bank.
- Unisa S., Sinh R., Prakasam C., 2002, “Sex selective abortions in India: evidences from two cultural settings”, Paper presented at the Symposium on Sex Ratio in India, January 2002, New Delhi.
- World Health Organization, 1999, Strategic and Policy Assessment of Abortion Services in Vietnam, World Health Organization.
- Zeng Y., Ping T., Baochang G., Yi X., Bohua L., Yongping L., 1993, “Causes and consequences of the recent increase in the reported sex ratio at birth in China”, Population and Development Review, pp. 283-302.

This article is available in open access under our model Subscribe To Open.